Sofema Aviation Services considers the exposures in Aviation Quality & Safety System Root Cause Analysis
Despite the best efforts of individuals and organizations to avoid negative outcomes serious adverse events will still take place.
RCA Techniques are essential within the Aviation Quality & Safety Environment both as a Proactive Tool as well as a Reactive Tool following an event.
When an event occurs, it is essential that we are able to act as professionals within our organizations, to assemble the facts, understand what happened and why it happened and to learn from such events and make appropriate changes to decrease the likelihood that such events will recur.
Benefits of Root Cause Analysis (RCA)
The principles of RCA can be applied to any real or perceived safety risk, near misses, and less severe safety events.
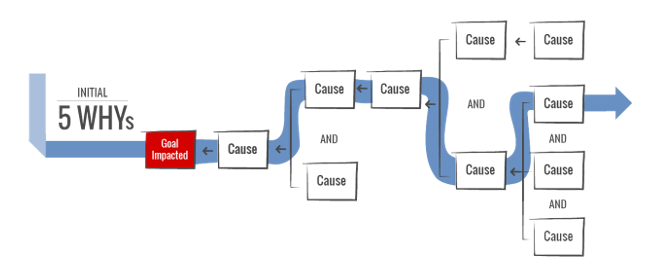
An RCA consists of three fundamental components:
(a) consideration and identification of factors most directly associated with the adverse event;
(b) analysis and prioritization of these factors to plan the introduction of effective strategies to prevent them from recurring and
(c) Development of Mitigation’s and the associated implementation management.
How to Make RCA Responsive & Effective in Your Organisation
1/ Within Organizations it is often difficult to engage with change management. Stakeholders will always be protective of “their” business areas and without senior support change management may be challenging.
2/ Look at the Bigger picture avoid the minutiae and start with the presumption that any person involved has delivered in the best possible way in consideration of the circumstances.
3/ Avoid biases and other emotions which may be inherent in the process or RCA Keep the report and discussions professional, objective, and non-judgmental.
4/ Having a RCA process technique is the key, we know serious adverse events will happen, so we should have a remedial process in place to deal effectively with the challenges.
5/ RCA can be extremely positive however if people and events are not treated diplomatically it may cause harm to individuals and organizations. Maintain confidentiality and, to the extent possible, anonymity identities should only be shared on a need-to-know basis.
6/ Recognize the RCA outcome and carry out the most effective mitigation which can be achieved with the availability of funds and if there is more still to be done identify this and record within the Quality and Safety Management system.
7/ Team members should include participating and responsible persons with the necessary competence to be able to effectively carry out all necessary steps related to the analysis and proposal for mitigation of the event.
8/ Effective communication processes should be in place to recognize or anticipate a potential problem and to have systems and processes in place for detecting such problems before or as soon as they occur.
Just Culture Approach
Within an existing culture of quality, all staff are encouraged to continuously be on the lookout for near-miss events and situations and to report these so that they can be addressed appropriately.
Confidentiality of the reporting and RCA processes must be maintained at all times. Maintaining a just culture is based on the willingness of all participants to share their observations, knowledge, and thoughts about actual and potential errors, which depends on an environment that is free from blame.
In an environment of blame, individuals tend to adopt a “code of silence” to protect themselves from shame, reprimand, termination, or even prosecution.
In a culture of safety, underlying system contributors are identified so that measures can be put in place to prevent a similar occurrence in the future, rather than blaming the most proximate individual.
The process of staff review should proceed with full confidentiality and respect for the privacy of all providers.
Nevertheless, consequences should be enforced in the rare cases of reckless behaviour, even in the absence of an adverse outcome.
Consider the following ground rules for the initial debriefing and subsequent meetings, which allow all participants to speak in a no-blame discussion of the decision-making process
Asking, “What factors are responsible?” rather than “Who is responsible?” helps to steer the conversation in the right direction.
Investigation Processes – Activity Steps
A detailed and thorough investigation of the adverse event facilitates the subsequent RCA process.
Building Ground Rules for RCA
Defining ground rules as part of the process will serve to drive the effectiveness of the process
The first question to address is, “What happened?” This is answered by putting together a timeline of the sequence event to objectively describe how the event unfolded, including the pertinent answers to the questions of “who, what, when, where, and how.”
The way in which this is presented may frame the investigation and management of the incident for months or even years to come.
Therefore, it must be done with great care and professionalism, defining each expected and actual step so that deviations can be identified readily
Measure, Collect, and Analyze Data to Identify Solutions to Address Root Causes.
Once the contributors have been identified, the focus turns to identifying solutions to address the root causes. The debriefing process requires gathering information from all involved parties through a facilitated review process.
To identify mitigation solutions and develop corrective actions, the contributing factors are measured, analyzed, and prioritized. By sequentially walking though the, path, and outcomes of the event, each step in the process can be documented and applied to a timeline.
The timeline sequence should map the incident to understand how such an event could logically have occurred. The goal is to prevent investigators from blaming specific individuals or jumping to conclusions. The timeline sequence (narrative) should be concise, relevant, objective and free from emotion or judgement. As far as possible, the narrative should de-identify the authors and all individuals involved in the event.
As an organization we need to understand why the event occurred and if it could happen with different persons involved (The substitution test)
Common tools applied at this stage include team brainstorming techniques and Pareto charts, which are visual representations and rankings of data collected from a cause-and-effect, or Ishikawa, diagram.
Consider which solutions can be implemented immediately and which solutions need preparatory work and resources and thus can be implemented only later.
Consider which solutions will require change in management.
The solutions to any problem depend on the circumstances and the spectrum of root causes.
Some technical contributors might be simple to remediate, whereas others might be more challenging and require greater effort.
For example, organizational causes may require development and implementation of a new policy, along with training and monitoring compliance with that policy.
Note – Human Factor contributors are the most challenging to remediate.
Sofema Aviation Services & Sofema Online provide Regularoty and Vocational courses including root cause analysis training. For additional details, visit our websites or email [email protected]

